

According to the American Society of Echocardiography, about 5 million people are affected by heart failure. 250,000 suffer from advanced heart failure with little or no response to medical therapies. And only About 2,500 people get a heart transplant a year.
Possible diagnoses that come with heart failure are valvular disease, ischemic disease, hypertensive heart disease, cardiomyopathy, pulmonary heart disease and pericardial disease.
When evaluating a patient for a heart failure, check for wall motion analysis, tissue Doppler, speckle tracking aka Strain for LV and RV contraction as well as M-mode.
What are LVADs and RVADs?
LVAD and RVAD are long term assist devices that act like a bridge to transplant, or recovery from acute myocarditis, Tako Tsubo or post MI shock. They can be used to maintain a normal cardiac output in patients with acute HF too (Otto, 2018).
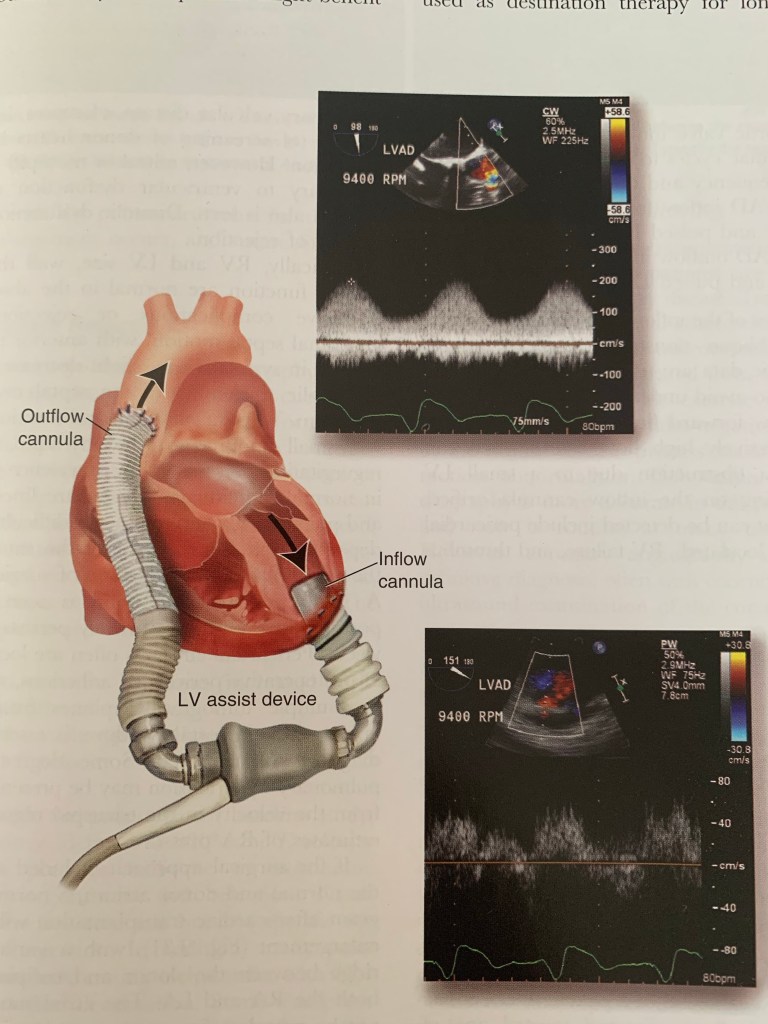
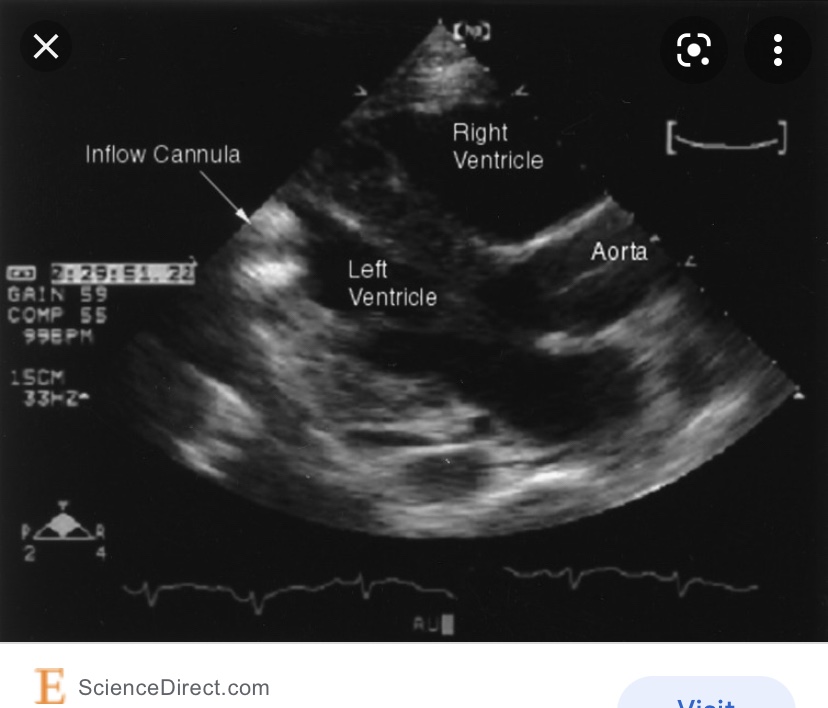
They consist of Inflow Cannula, Axial magnetic Rotor Pump and Cebtrifrugal propeller pump, outflow cannula (Aorta) and external battery (ASE).
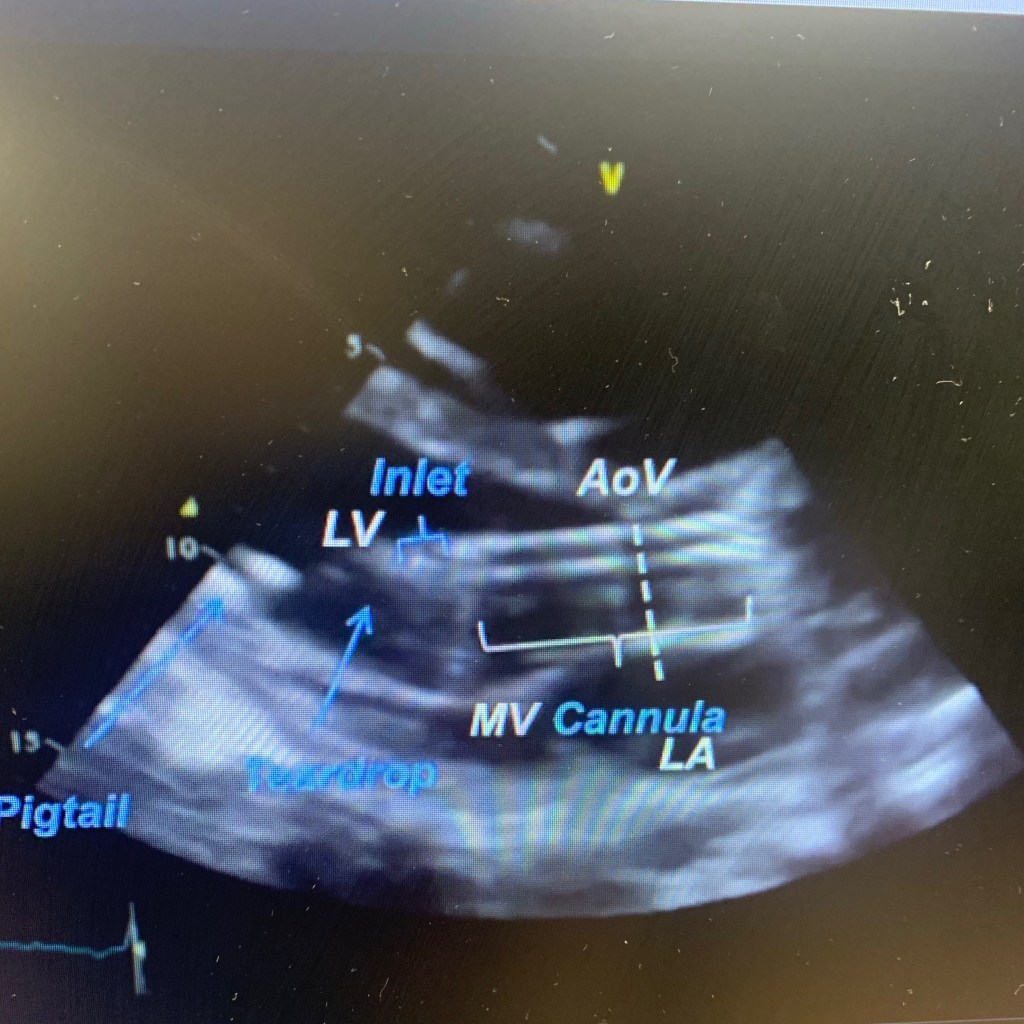
It’s hard to take pictures of either LVAD due to patients body habitus, post surgical dressings, stitches and supine position. Also, the flow is continuous. But when doing echo on LVAD patient, make sure you annotate the type, mode and pump speed. Take LV dimentions and measure EF by Simpson’s. Take pictures of aortic valve and run m-mode with reduced speed to 50mm/s, record LVAD inflow from apical conduit and use color and pulsed Doppler. And record outflow into the ascending aorta with dolor and PW. Make sure you take images (if possible) of the right heart, record any TR, visualize and take color and PW Doppler of IVC. And use color if needed to rule out any thrombus formation.
When performing echo on LVAD patient:
🔷measure RV systolic function(or dysfunction) and LV diastolic function (a diastolic dysfunction may indicate rejection later)
🔷 visualize and record any effusion around the heart
🔷 any wall motion abnormalities should be noted ex. Abnormal septal motion with anterior septal motion in systole
Selecting the right candidate
☑️left ventricle and interventricular septum: small LV size w/ increases LV trabeculation, LV thrombus, LV apical aneurysm, and VSD
☑️right ventricular dilation and systolic dysfunction
☑️ atria, interatrial septum and IVC: left atrial appendage thrombus, PFO or ASD
☑️ valvular abnormalities: any prosthetic valve with > mild AR, >= modetate MS or moderate TR or > mild TS, > mild PS and >= moderate PR
ASE guidelines- J Am Soc Echocardiography 2015;28:899-909
When to suspect LVAD thrombosis?
🔘right shift of the IVS and Enlarged LV
🔘 aortic valve opening with every beat (it should open every few beats)
🔘 blunted flow through both cannulas – use PW/CW
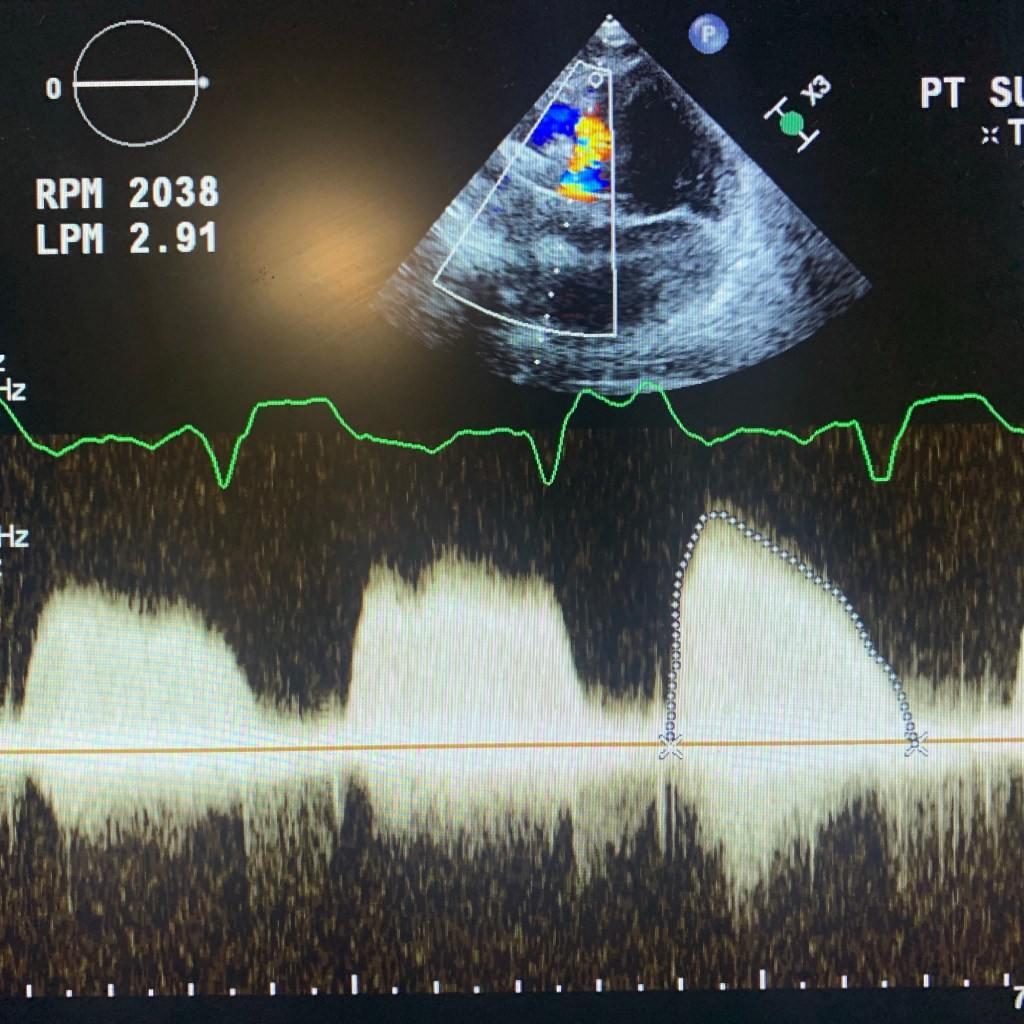
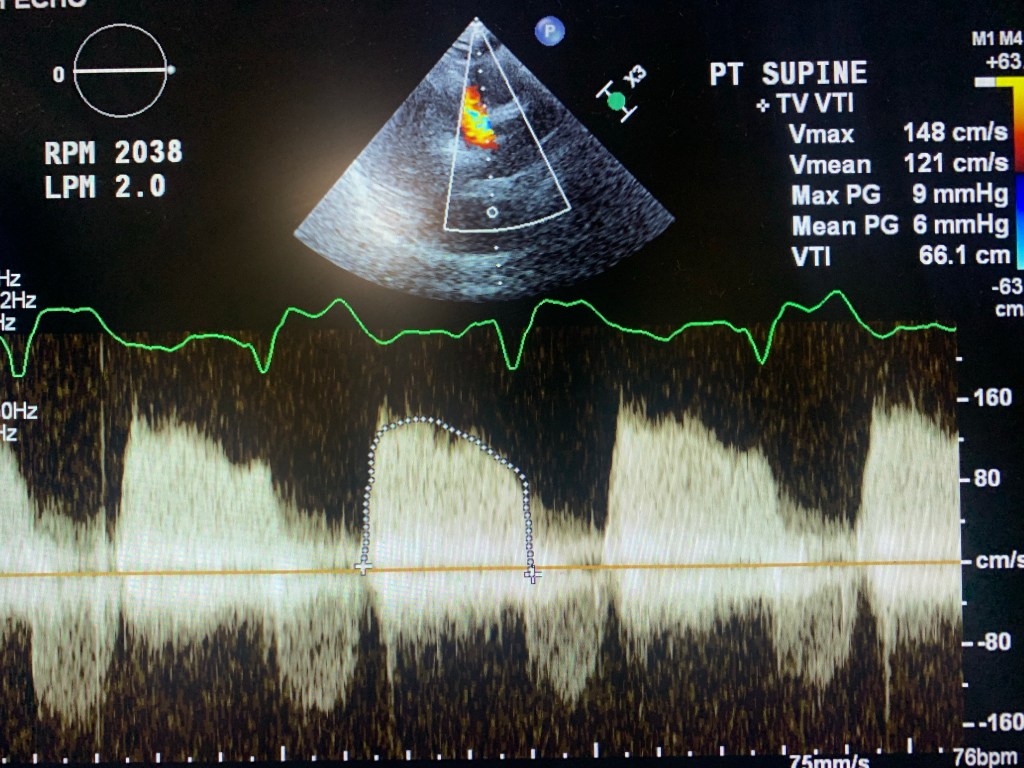
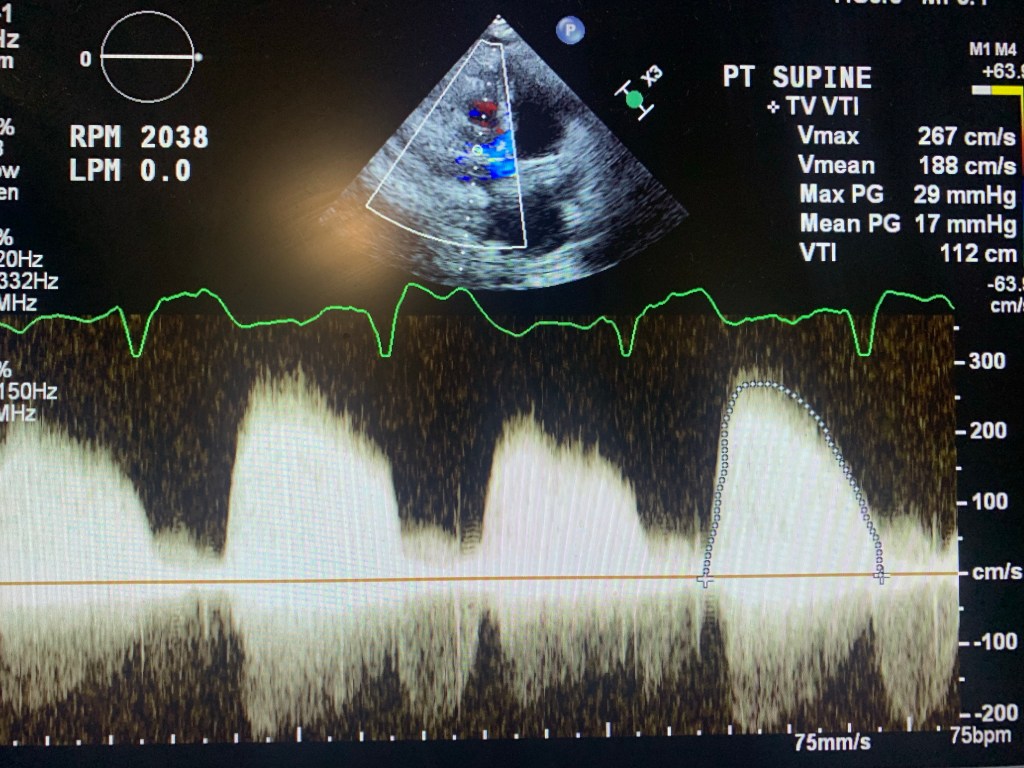
🔘 during RAMP studies: theres no LV dimention change with increased pump support/RPM
Please read more in ASE.org and Catherine Otto, Textbook of Clinical Echocardiography (2018)
Below are a few images and videos of RVAD and changes in RAMP study I did recently
Please let me know if missed anything to correct. I always want to provide correct information
